Be proactive: Delivering proactive care - Chapter four: Conclusions, Appendices & References
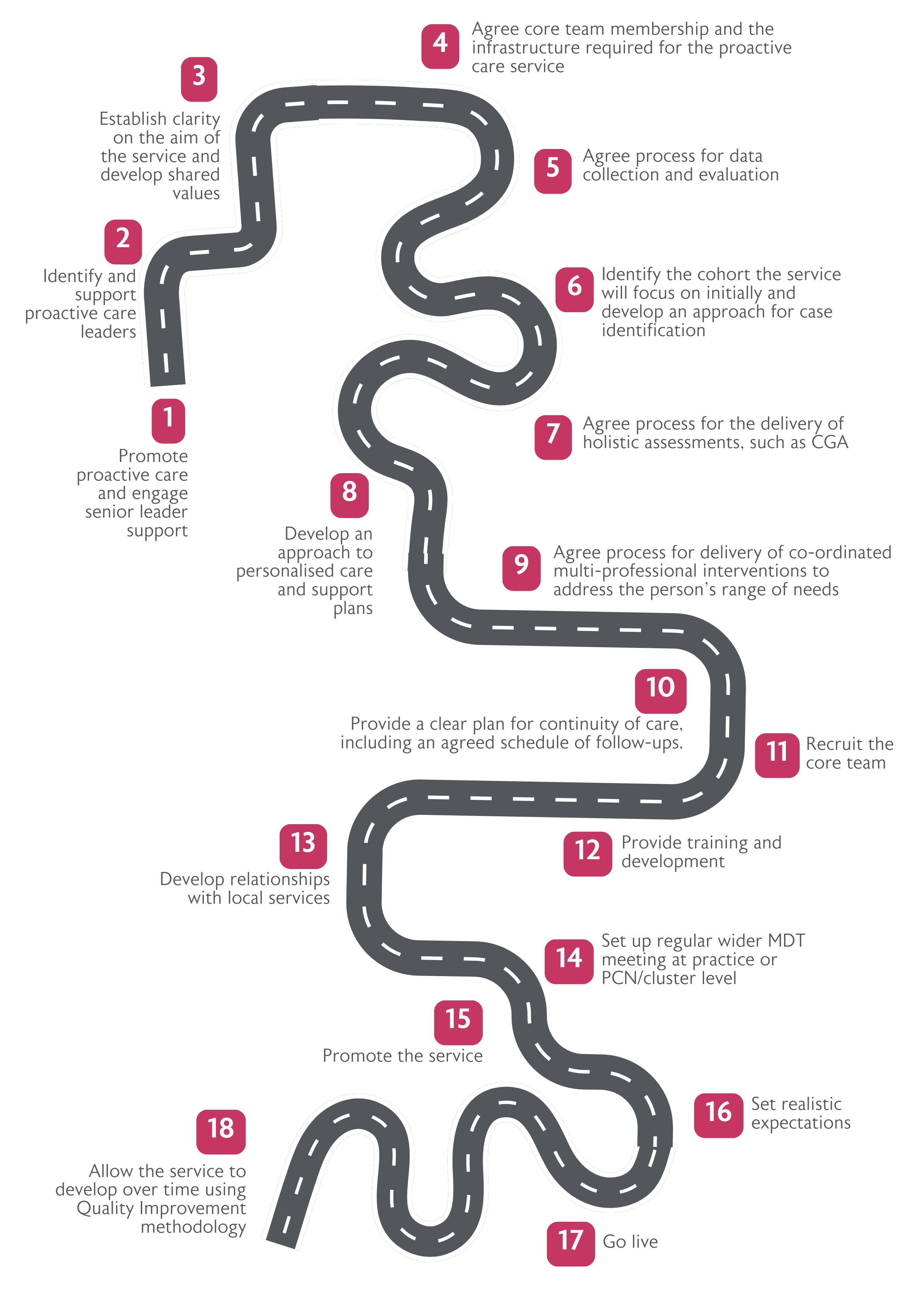
This publication outlines how to deliver proactive care against core components and key enablers, acting as a roadmap for implementing the NHS England framework and delivering proactive care services. This final chapter provides a conclusion, as well as appendices, including case studies of successfully implemented proactive care services.
Conclusion
With population ageing and older people living for longer periods with frailty, there is an increasing need for proactive care interventions to target older people with moderate and severe frailty to ensure they live well and stay independent for as long as possible.
Proactive care aims to be a cost saving approach which incorporates tailored and targeted interventions to ensure that the onset of poor health is delayed, individuals maintain independence, avoidable period of ill health are reduced, and older people enjoy healthier lives in the way the matters most to them. This prevents avoidable hospital admissions or readmissions, reduces length of stay in hospitals, and reduces the need for social care. It should be embedded across all community and primary care settings, and Co-ordinated funding and contracting is needed to ensure this becomes a reality.
Appendix 1: Examples of existing proactive care services
The BGS has collected a list of case studies from our members across the UK, illustrating existing examples of proactive care services in primary and community settings. The full list of case studies can be found here. The table below is intended to be guide for users to navigate to sample case studies of interest, depending on setting, pathway, and the type of advice sought.
|
Setting |
Name |
Pathway |
Does the case study include the voice of patients and staff? |
What were the main lesson learnt? |
What does the case study illustrate? |
|
One Primary Care Network |
Sport in confidence |
Led by one Occupational Therapist (OT) funded through Additional Roles Reimbursement Scheme. The OT leads on proactive frailty assessments and interventions. |
The case study includes patient stories. |
|
|
|
Single GP practice |
Caddington Surgery |
Team wide recognition of people with frailty needing assessment and management of long-term conditions. The service uses ARRS-funded roles. |
The case study includes patient stories and quotes from staff. |
|
|
|
Two Primary Care Networks |
North Devon Anticipatory Care |
MDT based proactive frailty assessment and intervention. It was a GP initiated community services collaboration which spread to a second PCN. |
The case study includes quotes from patients and staff. |
|
|
|
Primary Care Network and Community NHS Foundation Trust collaboration |
Moreton and Meols PCN and Wirral Community NHS Foundation Trust |
Shared PCN and community trust core team assess and follow up with patients with frailty identified through referrals and data searches. |
The case study includes quotes from patients and staff. |
|
|
|
One Primary Care Network |
Hatters Health |
Clinical Director initiated community trust collaboration operating across one PCN. Patients are identified through birthday card over 75 checks, proactive housebound frailty checks. It involves collaborative dementia support. |
The case study includes quotes from patients and staff. |
|
|
|
GP led collaboration with community services and acute trust. |
Islington PAWS |
System wide (acute, community, primary care) involving CFS screening for moderate frailty for proactive care. |
The case study includes a case story and quotes from staff. |
|
|
|
One Primary Care Network |
The PACT service, WISHH and 5 Lane Ends PCN |
Initiated by a community partnership (prior to PCN formation), which continued when PCN formed using ARRS funded roles. Individuals are identified through GP referrals and data. Home assessments are completed by upskilled care coordinators, followed by MDT review. |
|
|
|
|
Acute trust and single Primary Care Network collaboration |
Keeping Well Dunstable Hub |
The initiative is based in a newly built hub led by geriatricians. Care coordinators identify GP patients likely to benefit form holistic assessment and intervention. |
The case study includes staff and patients quotes. |
|
|
|
Three Complex Care Teams (CCTs) aligning with three Primary Care Networks |
South Somerset Complex Care Team |
CCTs consists of a GP, senior nurse, and band 4 support key worker aligning to a PCN. They provide comprehensive assessments of complex patients, coordination and information sharing with GPs, community teams, and secondary care hospital team. |
|
|
|
|
Three integrated hubs (each aligned with three PCNs) |
The North West Surrey Locality hub service |
Integrated MDT in three hubs receives referrals from any local health or social care professional within North West Surrey. Patients have to have a clinical frailty score of 4-8 and aged over 65. The hubs provide assessment, signposting, carer support, and follow up. |
The case study includes quotes from patients and carers |
|
|
|
Two Primary Care Networks |
Frimley |
Population health data is used to identify a cohort for frailty assessments by the MDT. Initially a geriatrician-initiated project in one PCN, which spread to two PCNs. |
The case study includes quotes. |
|
|
|
One integrated care centre covering 15 PCNs. |
Jean Bishop Centre |
Patients are referred to the centre which provides a comprehensive assessment from the MDT. |
|
|
|
|
Four GP Practices in collaboration with a local charity |
Lanarkshire |
MDT approach identifying patients through eFI and team knowledge to offer a holistic needs assessment to produce a care plan. |
|
|
|
References
References
Click to expand
- British Geriatrics Society, 2023. Joining the dots: A blueprint for preventing and managing frailty in older people. Available at: https://www.bgs.org.uk/Blueprint (accessed 30 September 2024).
- NHS England, 2023. Proactive care: providing care and support for people living at home with moderate or severe frailty. Available at: https://www.england.nhs.uk/long-read/proactive-care-providing-care-and-… (accessed 30 September 2024).
- British Geriatrics Society, 2024. Be proactive: Evidence supporting proactive care for older people with frailty. Available at: https://www.bgs.org.uk/ProactiveCareEvidence (accessed 30 October 2024).
- Molnar, F. and Frank, C.C. 2019. Optimizing geriatric care with the GERIATRIC 5Ms. Canadian Family Physician, 65 (1): 39.
- NHS England, 2019. The NHS Long Term Plan. Available at: https://www.england.nhs.uk/publication/the-nhs-long-term-plan/ (accessed 28 October 2024).
- Fuller C. 2022. Next steps for integrating primary care: Fuller stocktake report. Available at: www.england.nhs.uk/publication/next-steps-for-integrating-primary-care-… (accessed 12 September 2024).
- Whitty, C. 2023. Chief Medical Officer’s annual report 2023: health in an ageing society. Available at: https://www.gov.uk/government/publications/chief-medical-officers-annua… (accessed 17 September 2024).
- Han, L. Clegg, A. Doran, T. and Fraser, L. 2019. The impact of frailty on healthcare resource use: a longitudinal analysis using the Clinical Practice Research Datalink in England. Age and Ageing, 48 (5): 665-671.
- Scottish Government, 2017. Health and Social Care Standard: my support, my life. Available at: https://www.gov.scot/publications/health-social-care-standards-support-… (accessed 9 October 2024).
- Health Improvement Scotland, 2014. Ageing and frailty standards. Available at: https://www.healthcareimprovementscotland.scot/publications/ageing-and-… (accessed 9 October 2024).
- Welsh Government, 2014. Older people and people living with frailty: integrated quality statement. Available at: https://www.gov.wales/older-people-and-people-living-frailty-integrated… (accessed 9 October 2024).
- Northern Ireland Frailty Network. The Frailty Network. Available at: https://frailtynetwork.hscni.net/about-us/the-frailty-network/ (accessed 9 October 2024).
- British Geriatrics Society, 2023. BGS responds to long-awaited publication of proactive care guidance. Available at: https://www.bgs.org.uk/NHSEproactivecare (accessed 5 September 2024).
- Romero-Ortuno, R. 2015. Frailty in Primary Care. Interdisciplinary Topics in Gerontology and Geriatrics, 41: 85-94.
- Jones, H.E. Anand, A. Morrison, I. Hurding, S. Wild, S.H. Mercer, S.W. and Shenkin, S.D. 2023. Impact of MidMed, a general practitioner-led modified comprehensive geriatric assessment for patients with frailty. Age and Ageing, 52 (3).
- Hughes, L.D. Verity, T. Lawn, L. Gompertz, D. 2024. Proactive frailty in primary care: A primary care system fit for frailty. Journal of the Royal College of Physicians of Edinburgh.
- Arakelyan, S. Lone, N. Anand, A. Mikula-Noble, N. Lyall, M.J. De Ferrari, L. Mercer, S.W. and Guthrie, B. 2023. Effectiveness of holistic assessment-based interventions for adults with multiple long-term conditions and frailty: an umbrella review of systematic reviews. JBI Evidence Synthesis, 4(11): 1863-1878.
- Guo, Y. Miao, X. Hu, J. Chen, L. Chen, Y. Zhao, K. Xu, T. Jiang, X. Zhu, H. Xu, X. and Xu, Q. 2024. Summary of best evidence for prevention and management of frailty. Age and Ageing, 53 (2).
- Karunananthan, S. and Bergman, H. 2018. Managing frailty in primary care: evidence gaps cannot be ignored. Canadian Medical Association Journal, 190 (38): 1122-1123.
- Abbasi, M. Rolfson, D. Khera, A.S. Dabravolskaj, J. Dent, E. and Xia, L. 2018. Identification and management of frailty in the primary care setting. Canadian Medical Association Journal, 190 (38): 1134-1140.
- Bleijenberg, N. Drubbel, I. Schuurmans, M.J. Dam, H.T. Zuithoff, N.P. Numans, M.E. and de Wit, N.J. 2016. Effectiveness of a Proactive Primary Care Program on Preserving Daily Functioning of Older People: A Cluster Randomized Controlled Trial. Journal of the American Geriatrics Society, 64 (9): 1779-1788.
- Vestjens, L. Cramm, J.M. and Nieboer, A.P. 2018. An integrated primary care approach for frail community-dwelling older persons: a step forward in improving the quality of care. BMC Health Service Research, 18 (1): 28.
- Murtagh, F.E.M. Okoeki, M. Ukoha-Kalu, B.O. Khamis, A. Clark, J. Boland, J.W. Pask, S. Nwulu, U. Elliott-Button, H. Folwell, A. Harman, D. and Johnson, M.J. 2023. A non-randomised controlled study to assess the effectiveness of a new proactive multidisciplinary care intervention for older people living with frailty. BMC Geriatrics, 23 (6).
- Crocker, T. F. Ensor, J. Lam, N. Jordao, M. Bajpai, R. and Bond, M. 2024. Community based complex interventions to sustain independence in older people: systematic review and network meta-analysis, BMJ, 384.
- Bryce, C. Fleming, J. and Reeve, J. 2018. Implementing change in primary care practice: lessons from a mixed-methods evaluation of a frailty initiative. BJGP Open, 2 (1).
- British Geriatrics Society. Frailty Hub. Available at: https://www.bgs.org.uk/resources/resource-series/frailty-hub (accessed 7 October 2024).
- Lee, L. Patel, T. Hillier, L.M. Locklin, J. Milligan, J. Pefanis, J. Costa, A. Lee, J. Slonim, K. Giangregorio, L. Hunter, S. Keller, H. and Boscart, V. 2018. Frailty Screening and Case-Finding for Complex Chronic Conditions in Older Adults in Primary Care. Geriatrics (Basel), 3 (3): 39.
- Ambagtsheer, R.C.M. Archibald, M. Lawless, M. Mills, D. Yu, S. and Beilby, J.J. 2019. General practitioners’ perceptions, attitudes and experiences of frailty and frailty screening. Australian Journal of General Practice, 48 (7): 426-433.
- Mulla, E. Orton, E. and Kendrick, D. 2021. Is proactive frailty identification a good idea? A qualitative interview study. British Journal of General Practice, 71 (709).
- Health Education England & NHS England, 2018. The Frailty Framework of Core Capabilities. Available at https://www.skillsforhealth.org.uk/resources/frailty-2018/ (accessed 12 September 2024).
- British Geriatrics Society. Frailty elearning course. Available at: https://www.bgs.org.uk/elearning/frailty-elearning-course (accessed 8 October 2024).
- Royal College of General Practitioners, 2024. Introduction and overview of GPwER in frailty. Available at: https://www.rcgp.org.uk/your-career/gp-extended-roles/purpose-of-frailty (accessed 17 September 2024).
- Public Health Scotland, 2024. General Practice. Available at: https://publichealthscotland.scot/our-areas-of-work/primary-care/genera… (accessed 17 September 2024).
- Health and Social Care Scotland. HSCPs. Available at: https://hscscotland.scot/hscps/ (accessed 23 October 2024).
- Primary Care One. Cluster Area. Available at: https://primarycareone.nhs.wales/cluster-area/ (accessed 23 October 2024).
- Health and Social Care. GP Federations. Available at: https://online.hscni.net/our-work/gps/gp-federations/ (accessed 23 October 2024).
- Malone, S. and Hayes, M. 2017. Integrated Care Partnerships Northern Ireland - Leading Integration; Delivering Better Outcomes. International Journal of Integrated Care, 17(5): 1-8.
- British Geriatrics Society, 2023. The case for more geriatricians: Strengthening the workforce to care for an ageing population. Available at: https://www.bgs.org.uk/MoreGeriatricians (accessed 5 September 2024)
Contributors
Contributors
Click to expand
- Dr Lloyd Hughes, GP Partner, Tayview Medical Practice; and GP Lead for Primary and Preventative Care for Rehabilitation and Forensic Psychiatry, Stratheden Hospital, NHS Fife
- Dr Tara Verity, Portfolio GP with Special Interest in Frailty, Central Bedfordshire
- Dr Deb Gompertz, BGS Deputy Honorary Secretary; and Complex Care GP, South Somerset
- Dr Liz Lawn, BGS Honorary Treasurer; and retired GP
- Lucy Aldridge, BGS Policy Co-ordinator
Click to expand
With our thanks to the following BGS members who took part in three advisory board meetings to inform the content of this report:
- Dr Lucy Abbott, Consultant Geriatrician and Chief of Service for Community Services and Older Peoples Medicine, Frimley Park Hospital; and NHS England South East Regional Clinical Advisor for Frailty
- Dr David Attwood, Associate Medical Director, Livewell Southwest; Chair of the Healthy Ageing Programme Board, NHS Devon; and GP with Special Interest in Older People, Pathfields Medical Group.
- Dr Michael Azad, Consultant Geriatrician, Nottingham University Hospitals NHS Trust.
- Dr Eileen Burns, Former BGS President; and Former NHS England National Specialty Advisor.
- Anne Child, Pharmacy and Dementia Specialist Lead, Dementia Care Mapper.
- Emily Harrison, Senior Specialist Pharmacist and Independent Prescriber in Elderly Care and Frailty, Dorset County Hospital NHS Foundation Trust.
- Dr Adrian Hayter, Medical Director, Royal College of General Practitioners; and GP, Runnymede Medical Practice.
- Professor Anne Hendry, Senior Associate, International Foundation for Integrated Care (IFIC); Honorary Professor, University of the West of Scotland; Honorary Physician, NHS Lanarkshire Research and Development Department.
- Dr Rod Kersh, Consultant Community Physician, Partner, Manor Field Surgery, Maltby; and Divisional Director Therapies, Dietetics and Community Care, Rotherham NHS Foundation Trust.
- Dr Tessa Lewis, Locum GP, Wales.
- Aileen McCartney, Advanced Clinical Practitioner in Frailty, Whitstable Medical Practice.
- Claire Norman, Advanced Nurse Practitioner and Frailty Lead, Victoria Road Surgery, Worthing.
- Dr Marianne Plater, Community Geriatrician, Lymington New Forest Hospital.
- Dr Joanna Seeley, Specialist Doctor, East Kent Frailty and Home Treatment Service.
- Michael Smith, Specialist Nurse for the Older Adult, Market Rasen Surgery.
- Dr Jennifer Sutton, Project Lead (Council for Allied Health Professions Research), Royal College of Occupational Therapists.
- Dr Ana Talbot, Consultant in Medicine for Older Adults, University Hospitals Monklands; and Honorary Senior Clinical Lecturer, University of Glasgow.